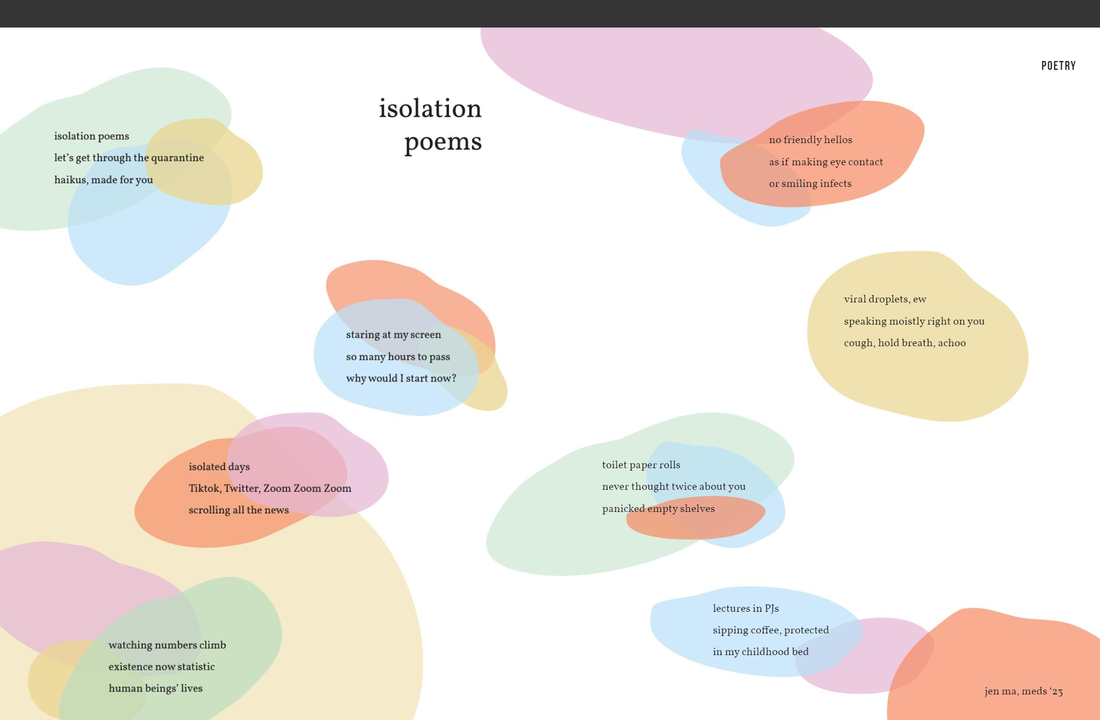
 Kind Exchanges in Cambodia
We started uneasy, adjusting Yet, every interaction came easy All kindness From every single person. “She wants to take us out to dinner.” Our instinct was to be scared We were advised to worry Yet, each person we spoke to Generous, overly generous Nothing we had seen before. “The laundromat fixed the hole in my pants without me asking.” Conversations were so different, The stories they shared Our normalcy, so dreamlike Their normalcy, hard to fathom Yet, all they spoke of was giving. Selflessly, regardless of circumstance. “She said ‘there is always someone who needs help.’ ” Finally, in moments of our gratitude They met us with confusion These kind exchanges, these are just their usual “He insisted on driving us everywhere.” “She hand-wove us gift baskets.” “He opened his house to us.” We the weary on the West, We have a lot to learn. - Iku Nwosu, Meds '22 Illustration by Kiera Liblik, Meds '23
0 Comments
 An inspiring story of how Queen’s medical, nursing, physical therapy and occupation therapy students united to help Kingston’s vulnerable populations
By: Valera Castanov, Meds '22 Introduction to KHealth When the COVID-19 pandemic first began, KHealth was among the few student organizations at Queen’s University that was able to rapidly respond and launch several initiatives to help Kingston’s vulnerable populations. KHealth started the Student-run Community Support Program, hosted “Call Your First Patient” Day and launched an emergency fundraiser for the Lionhearts Inc - a group that helps feed those in need in our community - raising over $2.4 thousand dollars. How did KHealth start and how did this organization end up at the forefront of helping our community during these difficult times? It all started with the author’s original idea of launching a student-run clinic in Kingston to help improve healthcare access to all residents of the greater Kingston area – particularly to the marginalized populations, and those without OHIP cards, permanent place of residence, official immigration status or with other limitations. Please see Queens Medical Review’s Issue 13.1 - Growth for a more detailed discussion. However, due to several logistical, financial, and legal concerns launching this clinic was not possible. When one door closes, another opens While working towards establishing a student-run clinic, the author was able to assemble executive and volunteer teams of interprofessional health students, gather community support and build close relationships with the administration. When the original idea did not work out, the author worked with all parties to develop a new vision and find a way forward to help Kingston’s vulnerable and underserved populations. This is when the idea of KHealth – Kingston’s Community Health Initiative was born. KHealth is the first student-led interprofessional community health initiative in Kingston, Ontario, where students from programs in medicine, nursing, physical and occupational therapy work together to improve the health and wellbeing of the local community. It is also the Class Project of Queen’s Medicine class of 2022! KHealth organization is actively developing educational and service-learning components, which are aimed to introduce students to working with vulnerable and underserved populations in an interprofessional community health setting. The organization also strives to combine theory and experiential learning to provide an enriching, immersive and interactive experience to students. Core values of KHealth are equity, diversity, and inclusivity. The organization aims to familiarize students to concepts of equity in healthcare and emphasize the crucial role of the social determinants on health and wellbeing. A large focus of KHealth is also on diversity and inclusivity. To date, KHealth has 14 executive team members and over 40 volunteers – each from diverse health programs, with diverse socioeconomic and sociocultural backgrounds – with a common aim to serve and be inclusive of everyone in the community regardless of their gender, age, race, sexual orientation, socioeconomic status, or overall health status. Overall, KHealth is positioned in a unique and fortunate position to be able to act as a liaison between the students in the Faculty of Health Sciences and the community and can leverage its volunteers and resources in the time of need. Consequently, when the COVID-19 pandemic first began, KHealth was able to respond quickly and launch several initiatives to help Kingston’s vulnerable populations. Please take a moment to read about some of KHealth’s COVID-19 initiatives below. KHealth’s Student-run Community Support Program Shortly after the beginning of the COVID-19, the KHealth’s Student-run Community Support Program (SCSP) was spearheaded by Queen’s medical students: Jenn Campbell, Vanessa Giuliano, Nia King, Ruchit Patel, Daniel Shi and the author, in partnership with students of the schools of Nursing (Michaela Patterson and Cici Siju), Physical Therapy (Kathryn McGuire and Justin Achat), Occupational Therapy (Grace Manalili and Theresa Fraser) and Medicine (Adam Gabara and Minnie Fu). The program involves partnering a student, from the Faculty of Health Sciences, with an elderly person and/or a member of a vulnerable population to assist them during the COVID-19 pandemic and beyond. The SCSP offers the following two services: 1. weekly check-ins via phone or video calls for social comfort; and 2. assistance with grocery shopping and delivery, medication pick-ups and/or minor tasks (e.g. picking-up laundry). All of KHealth’s volunteers have been instructed to follow strict COVID-19 precautions. Since the inception of the program, there have been 43 volunteer sign-ups and numerous requests for services from the community. The program was advertised in retirement homes, community groups, community health clinics and throughout the Faculty of Health Sciences. To date, SCSP volunteers have completed numerous grocery deliveries, phone calls and laundry pick-ups and drop-offs! The Kingston community has been overwhelmingly receptive to this program. Furthermore, KHealth was invited to present this initiative at the Ontario Medical Students Association’s COVID-19 Forum on Saturday, April 11th to partake in knowledge sharing with other medical schools in Ontario. It is projected that SCSP will continue its operations beyond COVID-19. “Call Your First Patient” Day COVID19 is an especially challenging time for seniors and vulnerable populations, and our First Patients, for the most part, belong to one or both of these groups. Consequently, KHealth hosted an inaugural “Call Your First Patient” Day on Saturday, April 4th, to encourage medical students to call their First Patients to inquire about their health and wellbeing, and ask whether they required any help or assistance of any kind. KHealth received a lot of positive feedback from both the participants and the First Patients. Some First Patients received numerous phone calls from different cohorts of medical students, one quoting that “[he] did not feel this popular in a while, it feels great”. Several First Patients also signed up for KHealth’s SCSP services. Overall, after having received a lot of positive feedback, KHealth will be suggesting to the Undergraduate Medical Education (UGME) to make “Call Your First Patient” Day a yearly event. Supporting Lionhearts Inc During the COVID-19 pandemic, the most vulnerable members of our Kingston community are disproportionately impacted. Several community organizations have significantly reduced their hours of operation or have been forced to close. In particular, this state of emergency severely exacerbated the food insecurity issues vulnerable populations already face. Among the organizations that are still operating during this difficult time is Lionhearts Inc. Every day, Lionhearts sets-up two mobile command centres, one in the McBurney Park (30 Alma St) and the other at the Weller Clinic (263 Weller Ave), and distributes nutritious meals and beverages to Kingston’s marginalized populations. Lionhearts also supplies warm clothing, personal toiletries, and fresh socks/towels. Most importantly, they provide a point of entry for those in need to access other emergency services. Lionhearts’ volunteers are some of the many heroes at the frontlines of the COVID-19 pandemic. However, due to the increased demand (over 240 people per day), as a result of closures in the Kingston community, Lionhearts needed help to continue their ground-breaking work. As KHealth believes in Lionhearts’ courageous efforts, a fundraiser was launched to provide financial contributions to support their ongoing projects. Within the first 4 days, KHealth was able to raise a total of $2,464! The fundraiser is ongoing, so please consider making a donation to support the Lionheats’ COVID-19 initiative. Final words KHealth is an inspiring story of how interprofessional collaboration can do a lot of good for the community. It provides an impetus to develop and support interprofessional education programs across all four schools in the Faculty of Health Sciences. KHealth proposes to collaborate with the Interprofessional Education Committee (IPEC) on the development of such programs. Acknowledgements The author would like to thank Canadian Federation of Medical Students (CFMS) for providing KHealth with the Community-Care Initiative Grant. Also, the author would like to extend sincere gratitude to the Ontario Medical Students Association (OMSA) for their COVID-19 Initiative Fund. Lastly, a huge thank you to The Aesculapian Society (AS) at Queen’s School of Medicine for their continuous logistical and monetary support. Without the help from all of these organizations, KHealth’s efforts would not have been possible. For more information: General information: khealth.info@gmail.com KHealth’s SCP: khealth.community@gmail.com Emergency Services and Food/Meal Programs Available in Kingston and Frontenac April, 2020 KHealth’s Student-run Community Support Program: Offering check-ins via phone/video call, grocery/pharmacy/foodbank delivery, and minor errands. Leave message at 613-817-7787 or email khealth.community@gmail.com Lionhearts: 263 Weller Ave. Take-home meals. 30 Alma Street. Take-home meals. Monday – Sunday, 5 – 6 p.m. Monday – Sunday, 6 – 7 p.m. Lunch by George: 129 Wellington St. Hot take-home meals or bag lunches. Monday – Friday, 11 – 11:30 a.m. Martha’s Table: 629 Princess St. Providing take away hot meals. Monday – Sunday, 11 a.m. – 1 p.m. Mutual Aid Katarokwi: Offering check-ins, grocery/pharmacy/foodbank box delivery. Leave message at 613-665-2959 or email mutualaidkatarokwi@gmail.com North Frontenac Food Bank: 14152 Road 38, Sharbot Lake Call 613-532-8855 for appointment. Partners in Mission Food Bank: 140 Hickson Ave. Please call 613-384-4534 for appointment. No walk-in service. Monday – Friday 8:30 a.m. – 12 p.m. and 1 – 4 p.m. Salvation Army: 342 Patrick St. Take-away prepared food baskets. Monday – Friday, 11 a.m. – 4 p.m. South Frontenac Community Services/Sydenham Food Bank: Frozen meals available for delivery daily. Hot meals delivered Tuesday and Thursday. Delivery only to South Frontenac/rural Kingston. 613-376-6477 St. Mary’s Cathedral: 260 Brock St. Providing takeaway light food/snacks. Monday – Friday, 1 p.m. – 4 p.m. St. Vincent de Paul: 85 Stephen St. Providing bag lunches. Food Pantry available by appointment Monday – Friday, 10:30 a.m. – 12 p.m.  By: Nicole Krysa, Meds '22
Current data suggests that in Canada 1 in 3 women and 1 in 8 men will be subject to unwanted sexual behaviour at some point in their adult lives. It is thought that this population might be even larger than is currently estimated, as the nature of the psychological sequelae following sexual trauma, as well as the stigma associated with being a “victim” means that many are reluctant to report or even acknowledge what they have endured. The implication of these striking figures for us as one-day physicians is that nearly all of us will encounter individuals who have suffered sexual violence in our medical practices. While many of these patients might want to discuss their current or historic trauma, they may perceive a barrier, assuming that their physician will not be understanding or receptive to what they have to say. In recognizing all of this, a universal symbol was created for physicians to display which signals to those who have been subject to sexual violence that they can make disclosures in a safe, trauma-informed environment. The current plan is to print this symbol on window stickers and pins, and to distribute it to physicians across Canada. In the meantime, we encourage physicians and other healthcare workers to employ it at their leisure, and to make others aware of it as well. Our hope is that it will be adopted and utilized universally. Thank you in advance for being an advocate against sexual violence and for supporting those in need. Logo Design Credit: Olivia Kotarba (www.okkdesign.com) References: Cotter, A., & Savage, L. (2019, December 5). Gender-based violence and unwanted sexual behaviour in Canada, 2018: Initial findings from the Survey of Safety in Public and Private Spaces. Retrieved from https://www150.statcan.gc.ca/n1/pub/85-002-x/2019001/article/00017-eng.htm  By Andrew Lee, Meds '22 Gone are the days when you tweeted about how boring second period calculus was, or showed the world your cafeteria lunch - #blessed. Twitter has gone through a revival since we last knew it, now becoming a forum for academic discussion, debate and trolling. #MedTwitter has taken the chirpy website by storm, amassing hundreds and thousands of tweets per day from all corners of the globe. Whether it be tweetorials or people straight meme-ing it, twitter has truly changed the way people in medicine interact with research, colleagues and the public. 1. Bite-sized information in real-time Twitter is not for the faint of heart, it is a constant barrage of information. However, in 140 characters people are forced to be concise. The only atrocity is verbosity. One can receive up to date information from reputable sources at their fingertips. With trending hashtags and the opportunity to go “live” twitter has built an ecosystem conducive to digestible information. To optimize your twitter experience you can set up lists, follow certain hashtags and obviously follow your favourite influencers. Twitter is the Costco sampler of the internet. 2. Breaking down barriers with mentors and idols Academia has always been inaccessible, the coveted “cool kids table” in the cafeteria. However, twitter has been able to bridge the gap between the nerds and jocks. Liking, replying and retweeting your idol’s tweets is an opportunity to be seen. There is a low threshold to echoing the voices of others on this platform and if you appear in someone’s feed enough, they might just send a follow your way. It’s like having your professors and heroes on Facebook, but in a more professional manner. This is a great way to connect with people you find interesting or inspiring and it breaks down the intimidation of sending a formal email. Not to mention, this humanizes your idols. You learn about their quirks and interests and you can see their “likes”. Why yes, professors also enjoy the occasional meme. 3. Subcultures Like any good social media platform, subcultures exist. From #gaymedtwitter to #medhumchat you can explore niche areas of medicine that might not be prominent at your home institution. This allows you to connect with people around the world who share marginalized identities or specific interests tangential to medicine! There is so much to offer and medicine is so much more than… well medicine. Look hard enough and you will find the #HotDogIsASandwichDoctorsClub, even though that opinion is straight up wrong. 4. Being vulnerable Although Twitter has become a professional forum, it has still retained some of the personal nature of what we once knew. From your tough days to angry rants, many physicians can be quite vulnerable on the platform. Especially in the era of COVID-19, we see across the board an unprecedented vulnerability displayed by colleagues. I for one, believe that this is healthy for medical culture. It is important to show our colleagues, learners and society at large that physicians are prone to similar stressors (if not more) as everyone else and sometimes, life is just plain ol’ hard. Thank you for all the doctors out there who have shown us that being vulnerable is not a weakness, but a strength. 5. Meme-ing it From Dr. Glaucomflecken our resident eyeball enthusiast and tiktoker, to sassy memes by accounts by the self-proclaimed monikers such as HotGirlMed or BlondeBoy3000MDToBe. The anonymity that Twitter provides can be an outlet for disgruntled medical students around the globe. Dark humour has always been a part of medicine - this is just the modern form.  By Jessica Nguyen, Meds '23
I grew up hearing that “I’m very lucky”. As a first-gen Canadian and a daughter of two refugees, I knew that I would never know adversity like my parents do. Yes, I heard stories of about their life-altering journeys from war-torn Vietnam to Canada, but I don’t think I ever really took a minute to marvel at the strength, courage, and sheer luck that it took for my parents to make it to this country. That is, until a simple conversation we shared while on a drive to Kingston. In the midst of the COVID-19 pandemic, my dad and I were on the road to pack up some things so I could move back home. We ate snacks in the car, listened to music, and talked about how lucky we are to have a house to socially distance inside, full of cupboards of food and closets of board games to distract ourselves. My brother had just turned thirteen that week. Curious about what my father’s life was like at thirteen, I asked him about his upbringing and journey to Canada, something he rarely talks about. During my father’s childhood, Vietnam was still recovering from a war that still has grips on the country today. My grandfather was a soldier for the side that lost the war and was branded a ‘traitor’ after it ended. He was imprisoned and my father’s family was forced to move to the southernmost province of the country. “It was riddled with malaria and water-borne diseases,” he told me. “They made us live somewhere that was basically a jungle, and we survived there for five years. Essentially, the government oppressed anyone who had stood in its way during the war.” He was three years old when the government moved them. Five years later, his family moved back to the city, where they survived on the streets. At least there was opportunity to find work there. Back then, living on the streets was the norm for families that had fought for the “wrong side” during the war. After all, they lost everything. “We were so poor,” my dad told me. “We had this wooden fish that we would put on a plate to make it seem like we were eating more than just a bowl of stolen rice for dinner”. Living in the city, my father made a friend who eventually presented my father with an opportunity to flee the country by boat. In the years after the war, millions of Vietnamese citizens fled the country this way in hopes of finding a better life, and at the age of fourteen, my dad became one of them. Not only did he face the dangers of the sea, he also faced death – escaping was a crime that the government persecuted many people for, with countless dying these journeys. When my father told his parents that he was planning on escaping, my grandmother insisted that his older brother take his place on the boat instead. My uncle was almost at the age of conscription and she didn’t want him being taken away by the government. My dad begrudgingly agreed. The night of the planned escape, my dad stayed awake all night, until he heard his brother leave quietly to go to the meeting point. “I decided last minute that I was going on that journey no matter what, so I jumped out of the window and followed your uncle in his xích lô to the meeting point”. He ran after my uncle for 15 km through the night to the first meeting point, where they would meet others that were headed onto the same boat. When my uncle realized that my father had been following him, he demanded that he return home. “I was getting on that boat no matter what,” my father said. When their small fishing boat left the dock, the police had caught wind of the escape. “They shot at us until we crossed into international waters,” he recounted. And then when they were just barely safe, they realized that their motor had fallen off in the commotion. “All forty-four of us thought we were going to die. During the day all you saw was water and during the night, you couldn’t see anything. How was anyone going to find us?” he said. “It was so cold I went to sleep in the boiler room one night and had some oil spill on me. It would keep me warm during the night, but I didn’t realize how terrible of an idea it was until the morning, when the sun would burn my skin”. Not only that, they suffered from dehydration, starvation, and seasickness. I don’t know how he held onto hope after being at sea for seven days. On the seventh day, a terrible storm was headed straight to them. My father looked up at the sky wondering how his life could end this way. “I regretted everything. Being a troublemaker to your grandma, leaving home without telling anyone, not trying harder to help around at home”. Everyone cried and prayed. It seemed that they were just going to be another failed attempt at escape, a shipwreck containing bodies of passengers that never made it to freedom. But out of sheer luck, an American ship found this tiny fishing boat in the middle of the ocean and brought them to the shores of Singapore. They were saved. From the Singaporean refugee camp, my uncle sent letters back home and told my grandmother he was safe. She wrote back, telling him she was heartbroken that my father was lost and had run away from home. Imagine her surprise when she found out he was with my uncle all along! After a couple months at the camp, my father and uncle arrived in Canada. (Fun fact: they chose Canada because the snow looked so beautiful – ironically, they are both the biggest grouches during Canadian winters nowadays). Two young men, fourteen and twenty-one, starting their lives in a country whose language they didn’t speak and customs they didn’t know. It amazes me how refugees like my father manage to build a life in Canada despite all odds. While other teenagers spent their time playing video games, my father spent his years learning English and trying to sponsor the rest of his family to Canada. While others lived their lives oblivious to what was happening in Vietnam, my father and countless others rebuilt their lives in countries they had never heard of before. So, there I was. Listening to this insane story, in disbelief at how the man driving the car, who I call ‘dad’, had risked everything in hopes of a life he would have never dreamed of. I couldn’t believe that this man eating a whole bag of mini eggs with me, was also a man who was able to journey to another country, learn its language, and thrive in its society at the age of fourteen. I don’t know why I had never had this conversation with my dad before, but I knew that this would forever change how I see the world. When I hear “I am lucky”, I know that it is true. After all, it was only one generation ago that my family had to risk their lives for the hopes of a brighter future. By Valera Castanov, Meds '22
Plastic and reconstructive surgery is a versatile specialty with a great diversity of subspecialties, surgical techniques, conditions treated, and the ability to transcend multiple anatomical boundaries which restricts other surgical disciplines [1-4]. However, due to its versatility, the exact scope of plastic and reconstructive surgery is often not well understood by the public and other healthcare providers [2-4]. The media further exacerbates the misunderstanding by portraying plastic surgeons as primarily aesthetic (cosmetic) surgeons, while neglecting other subspecialties within the field [1,4]. This article will discuss some subspecialties within plastic surgery to shed light on non-aesthetic procedures and showcase the great diversity available in plastic and reconstructive surgery. Reconstructive surgery includes breast reconstruction, burn, craniofacial, hand, and oncology surgery. Breast reconstruction Breast reconstruction is a surgical procedure aimed to restore the appearance of a breast, most often after a mastectomy, lumpectomy, or trauma. For patients undergoing a mastectomy or lumpectomy, breast reconstruction can be performed at the same time (immediate reconstruction) as the surgery to remove the affected breast tissue, or at a later time (delayed reconstruction). Different techniques of breast reconstruction exist, which include alloplastic and autologous reconstructions. Alloplastic breast reconstruction involves using an implant, whereas, autologous technique uses the patient’s own tissues to restore the breast. Autologous reconstruction is also called “flap” reconstruction, as a “flap” refers to the transfer of tissue from one area of the body to another e.g., abdomen to breast. Plastic surgeons can also decide to do combined techniques, using both the patient’s own tissues and an implant. Burn surgery Plastic surgeons are involved in the treatment of burns and perform acute and reconstructive surgeries. Acute burn surgery occurs immediately after the injury and includes surgical excision and skin grafting of deeper burn wounds. Reconstructive burn surgery takes place following the healing of burn wounds, with the goal of improving function, comfort, and appearance. Craniofacial surgery Craniofacial surgery is a surgical subspecialty that deals with the cranium and the facial skeleton, along with the overlying soft tissue. This subspecialty is further divided into adult and pediatric surgery. Adult subdivision focuses primarily on trauma and post-traumatic craniomaxillofacial deformities, orthognathic surgery, orbital defects, and a variety of other craniofacial bony and soft tissue pathologies. Pediatric craniofacial surgery deals mostly with congenital malformations of the craniomaxillofacial skeleton and soft tissue, which include craniosynostosis, cleft lip, cleft palate, craniofacial cleft, micrognathia and many others. Hand surgery Hand surgery deals with the management of acute, chronic and congenital conditions of the hand and wrist. It involves the treatment of different regional body tissues, including skin, ligaments, tendons, vessels, nerves, and bony structures. Plastic surgeons perform tendon repairs/transfers/releases, fracture repairs, reconstruction of injuries and other deformities. Hand surgery involves the management of conditions such as the carpal tunnel syndrome, trigger finger, dupuytren’s contracture and many others. Microsurgical techniques are used in many procedures, e.g., replantation surgeries of the traumatic hand and digit amputations, for nerve and soft tissue reconstruction and blood vessel re-connection. Oncology surgery Plastic surgeons treat different types of skin cancer, including basal cell carcinoma, squamous cell carcinoma and melanoma. Surgical approach depends on the type, extent, and location of the skin cancer, along with other factors. Some procedures may require flaps or skin grafts. One of the most sophisticated skin cancer surgeries is Mohs surgery. It involves removing the visible portion of the cancerous skin lesion, along with the thin layer of tissue deep to it. The excised deeper tissue layer is then mapped, and a histological analysis is performed. If cancerous cells are detected, the next layer of skin is excised from the affected area and analyzed. The procedure is repeated until cancerous cells are no longer present on microscopic examination of the biopsied tissue. Aesthetic surgery Aesthetic (cosmetic) surgery is a subspecialty of plastic and reconstructive surgery, which focuses on enhancing a patient’s appearance. It is an elective surgery, with the goals of improving appeal, symmetry, and proportion of a part or a region of the body. There are numerous aesthetic procedures that can be performed, which focus on facial and body contouring and rejuvenation. Discussion of individual procedures will be the topic of a separate article. Conclusion Plastic and reconstructive surgery is one of the most diverse surgical fields that medical students can pursue. Despite the media focusing primarily on aesthetic surgery, it is just one of the many subspecialties of plastic and reconstructive surgery. Plastic surgeons operate on different parts of the body, use versatile approaches from macro- to microscopic techniques, treat diverse patient populations - from pediatric to geriatric patients - and work within interdisciplinary teams to deliver comprehensive patient care. The diversity within this surgical field is truly fascinating! Disclaimer: The list of subspecialties mentioned in this article is not all-inclusive, and highlights only a few of the many surgical techniques and approaches used by plastic surgeons. Some of the surgical techniques specified for individual subspecialties, e.g. microsurgery for hand and/or digit replantation, can be used across many different subspecialties. Of note, plastic surgeons often work in large interdisciplinary health teams when treating many of the above-mentioned conditions. For the purposes of this introductory overview article, many things were simplified. [1] Agarwal JP, Mendenhall SD, Moran LA, Hopkins PN. Medical student perceptions of the scope of plastic and reconstructive surgery. Ann Plast Surg. 2013;70(3):343-349. doi:10.1097/SAP.0b013e31823b6c19 [2] Kim DC, Kim S, Mitra A. Perceptions and misconceptions of the plastic and reconstructive surgeon. Ann Plast Surg. 1997;38(4):426-430. doi:10.1097/00000637-199704000-00020 [3] Fraser SJ, Al Youha S, Rasmussen PJ, Williams JG. Medical Student Perception of Plastic Surgery and the Impact of Mainstream Media. Plast Surg (Oakv). 2017;25(1):48-53. doi:10.1177/2292550317694844 [4] Dunkin CSJ, Pleat JM, Jones SAM, Goodacre TEE. Perception and reality-a study of public and professional perceptions of plastic surgery. Br J Plast Surg. 2003;56(5):437-443. doi:10.1016/s0007-1226(03)00188-7 By Emma Spence, Meds '21
Aware that many would not be eager to dive into an article about Feedback, I knew that I would need to do something to captivate your attention. I hope to entice you to stay tuned at least long enough for me to share my view on feedback. Come my third year of medical school, I now realize that feedback is one of the most significant contributors to my growth and development as a burgeoning clinician. How uniquely valuable it is that I get to glean opportunities to see myself through expert eyes, to get practical insight from MDs with decades of experience, and to get an honest rating of my performance. Since I have come to value its importance so highly, I have invested significant thought into breaking down my approach to feedback, some aspects of which I hope to share here. Feedback in medical training comes in many forms. It can look very different based on the individuals involved, the level of training, the setting in which it was evaluated and received, etc. While a sit-down meeting can be conducive to communication, sometimes a telling gaze across a room can send all-too-clear a message. Feedback can be an expressive process through exchanges with others. However, it can equally be an introspective and reflective practice carried out within one’s own consciousness. While many of these may be simultaneous and ongoing, various individuals tend to weigh differently the value of spontaneous versus elicited feedback, external versus internal feedback, and verbal versus non-verbal feedback. I believe that it is crucial to tune into all of these forms of feedback in order to optimize one’s development as a medical learner. For the purposes of this article, I will focus on elicited verbal external feedback. I recall learning about giving and receiving feedback during the Clinical Skills course in my first year of medical school. While this learning did effectively prompt me to shift away from my previously employed “compliment sandwich” method of receiving and delivering feedback, the content felt fairly intuitive and conceptual, and I did not think too much it. It was not until clerkship that I really experienced what it was like to receive poor quality feedback. I don’t mean feedback telling me my performance was poor - I have gratefully received constructive feedback throughout my training. Rather, I mean feedback that was poor in that it did not help me to assess my performance in a way that would be useful to my development as a learner. Some assessors would clearly have intentional, organized, pertinent and thoughtful methods of giving feedback. Contrastingly, others would simply employ the “things are fine” approach. The latter would sometimes make me mourn the wasted breath – my words in eliciting the feedback would seem futile, and I felt almost guilty having them expend their breath on an unconstructive answer. Both of these types of experiences have prompted me to appreciate that creating valuable feedback is in fact a skill –a skill that not everyone has been explicitly taught. I would like to emphasize here that I have yet to even mention the content of any feedback. This discussion has little to do with whether the feedback received is positive, constructive, or otherwise. Rather, it has to do with how effectively feedback can be elicited, delivered and received by students – the performance quality of the skill of feedback itself. Once I established that feedback was a key component of my learning, I decided that it was a worthwhile investment of my time. The trouble was, external feedback inherently involved individuals and elements beyond my own locus of influence. So, came the understanding that in order to acquire the caliber of feedback I sought, I would have to make the most of those things that I could in fact control. Below are a series of questions I now tend to ask myself each time I seek out verbal external feedback. As with most things, there is certainly more than one good way to approach feedback. I hope to share just one such method that I have personally found to be constructive in case a colleague might derive benefit. Why do I want this feedback? There are instances where we collect feedback simply because we have to, or because we feel we should. For example, at the end of a Clinical Skills encounter during pre-clerkship or to fill out one of the tens of clerkship evaluations we are all unavoidably required to submit. Beyond the program requirements, however, I find it valuable to take a moment to consider why ‘I’ want this feedback. There are occasions when we seek others’ thoughts as a means of forcing ourselves to reflect on our own performance. Alternatively, asking for a performance evaluation can force an assessor to reflect critically on our functioning, which may be valuable to get their wheels turning with regard to a reference letter, to reflect our investment as a learner, or to somehow implant ourselves in their memory before getting lost as yet another clerk rotating through their service. Sometimes we ask for feedback simply to ensure that we aren’t doing a terrible job! Often, opening a feedback discussion carries the intent of debriefing – whether about an isolated difficult encounter or a longitudinal clinical experience. Other times, admittedly, we are looking for some reassurance or a pat on the back. Evidently there is a wide variety of reasons we might seek out feedback. Program requirements and reassurance aside, if I can truthfully say that my motivation to receive this particular feedback is due to a genuine desire to improve, then I can move forward to these following questions. What am I willing to put in to receive high quality feedback? As is frequently the case, “you often get out what you put in.” External feedback is a conversation, which inherently involves at least two people. As such, if we are expecting meaningful output from them, it is only fair that we input a similar amount of thought and effort. The timing of a request for feedback is important. In my opinion, if I catch a preceptor with one foot out the door on a Friday afternoon to ask for feedback, it would not be fair of me to be frustrated with a low-volume, generic response. While there is only so much control we can exert over the ever-unpredictable schedules of clinicians, one thing I do to help myself is to foreshadow my desire for a discussion. This typically helps us to later find a time and place that feels more private and less rushed. It is equally important to make sure you have provided the assessor with the information they require in order to give valuable feedback. After pre-clerkship, oftentimes it is challenging for staff to keep track of your level of training – did that clerk say they were in third or fourth year? Does their school have a fourth year? Does that mean they have only done core blocks or elective placements? Why do they need this feedback? Is it simply to review whether the course objectives were satisfied or is it because this particular rotation is important regarding career choices? You know your own training, experiences and goals better than anybody else. So, I have found it really helpful to voice what my own objectives and focus-points are, which provides specific things for my assessor to comment on that are actually valuable to me and appropriate to my level of training. A final, very valuable, input of effort prior to seeking feedback is self-reflection. This reflective process can be quite brief. For instance, if you only worked with a staff for one day, there is not a lot to review. However, if you have worked with someone over a longer period of time, it can be a deeper dive into how you feel you have developed over recent days, weeks, blocks, etc. I have found that going in with my own assessment of my learning and performance adds meaning and calibrates whatever is subsequently shared with me. I have often found it helpful to voice these reflections (negative, positive or otherwise) to my assessor prior to them sharing their thoughts as it provides a framework as to the scope, depth and topics of commentary I am hoping for. Are there considerations I need to make from the other person’s point of view? Most teachers do in fact want to stimulate and contribute to the growth of their learners, and many see feedback as a key component of this process. However, it is important for us students to consider that while we are there to learn and grow – other than in controlled setting such as clinical skills or a classroom – our superiors are there to care for and keep patients alive. As such, we must be cognizant of the setting, timing and emotions surrounding our desire to learn. Also, when it comes to viewing things from another’s perspective, I would like to openly admit that my assessment from others’ points of view with regard to feedback has more than once been quite inaccurate – thinking a week was going terribly but finding out at the end this staff was impressed by how much he pushed me. This to say, while it is courteous and important to consider things from another’s viewpoint, avoid losing learning opportunities by shying away from seeking feedback from individuals when you think you already know their opinions. You will often be surprised how differently they see things. How am I going to respond to this feedback? Responding to feedback is often a two-part process involving both an immediate and longer-term response. In the moment, feedback can spark any number of emotions from flattery, to embarrassment, to frustration or disappointment. This aspect of feedback likely is the most disparate in terms of how individuals handle themselves. One approach is to allow yourself to feel whatever emotion is stirred up in that instant, while still allowing yourself to listen to all the feedback being offered. It would be a wasted effort to go through this whole process only to not listen to what your evaluator has to share. Once the encounter has passed, you are then able to select what information you would like to carry forward with you versus what information you might leave behind. Yes, you are allowed to leave some comments behind. However, I would caution that comments which I have found myself feeling defensive about in the moment, have turned out to be some of the greatest motivators or contributors to my growth. Ultimately, how you respond to the feedback ties in extremely closely with my first question – Why do I want this feedback? If I did genuinely seek this feedback in order to grow, then I will want to jot down the information that has been shared with me and apply the feedback that has been given. ---- As mentioned throughout, these questions are by no means strict choreography to successful exchanges of feedback. These are simply some thoughts to consider as we go through our medical training that undoubtedly will be inundated with feedback (sometimes to the point of “feedback fatigue”). Ultimately, despite our best efforts, there will still be occasions where all we get back is, “things are fine” – and that is ok. I feel that if I have carried out this exercise and asked myself these questions, I have done my part in the dance of feedback. While the dance may have turned into a solo, I will have, nonetheless, invested truly meaningful reflection that contributes to my ultimate goal of growth.  By: Kassandra McFarlane, Meds' 23
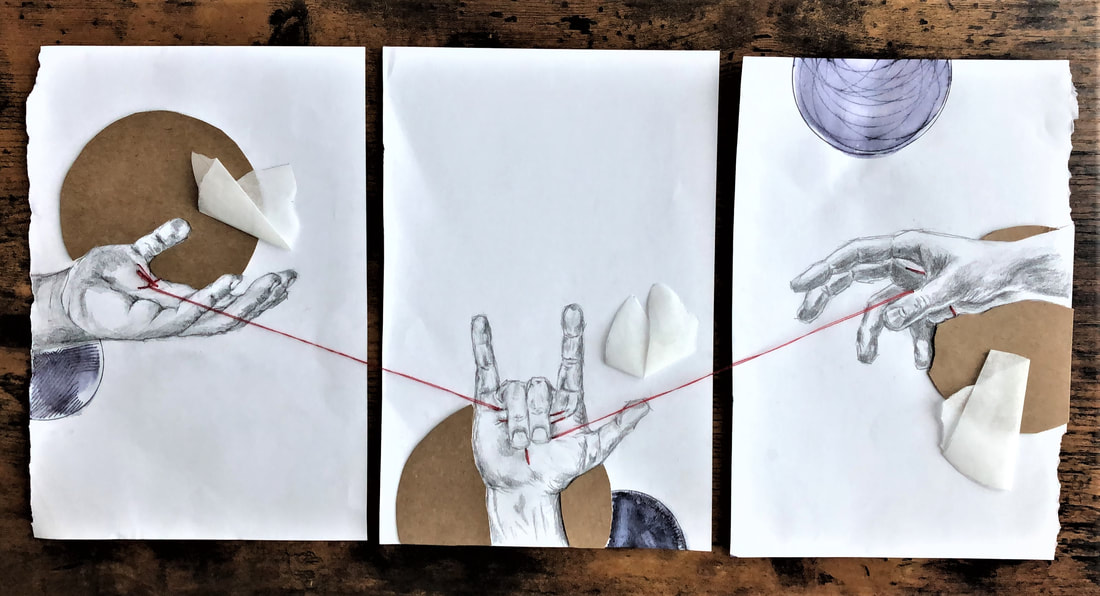
Like many others in the past few weeks I find myself in unfamiliar territory. The upheaval in my life in light of this global pandemic has been a creeping escalation. Naturally, as the severity of this new virus became more apparent and government-initiated social distancing came into effect, I felt less secure in the routines I had grown accustomed to because they were no longer available to me. I feel disjointed – half of my life in Kingston and half of it in Vancouver. I am living out of a suitcase; I left Kingston with the intent to be absent for one week. It has been nearly four. I haven’t seen my parents or my friends for months and I am uncertain of how the next months of my life will unfold. My future is anything but certain. From this upheaval, though, has arisen a new motivation and inspiration for creativity. I have written more short stories than I ever have and have also started co-writing a novel. I feel more in tune with my penchant for expression and notice that I am more willing to engage my creative urges. Most recently, after exploring a local park nearby, I noticed a large cherry tree in bloom with full blossoms erupting from every branch. I was struck with inspiration for a photoshoot (the result of which is the adjoining image to this brief reflection). There is a stillness of thought in the flow of a creative endeavour; fully engaging allows us freedom to relegate the tough parts of life for a moment. Though the current global situation is tumultuous and at times frightening, I have found resilience by following my intuition and spontaneous drive to delve into creative projects. Art allows us to pause and reconnect with our inner worlds and find comfort in our own self-expression. My life is confusing right now, as is true for all of us, but we have control over the allocation of our attention and the things we choose to focus on. By returning to ourselves and finding ways to stay present-focused, we will weather this storm and emerge with deeper self-knowledge, both individually and collectively. Photo credit: Tyler Skode |
In This Issue:
All
|

 RSS Feed
RSS Feed
