|
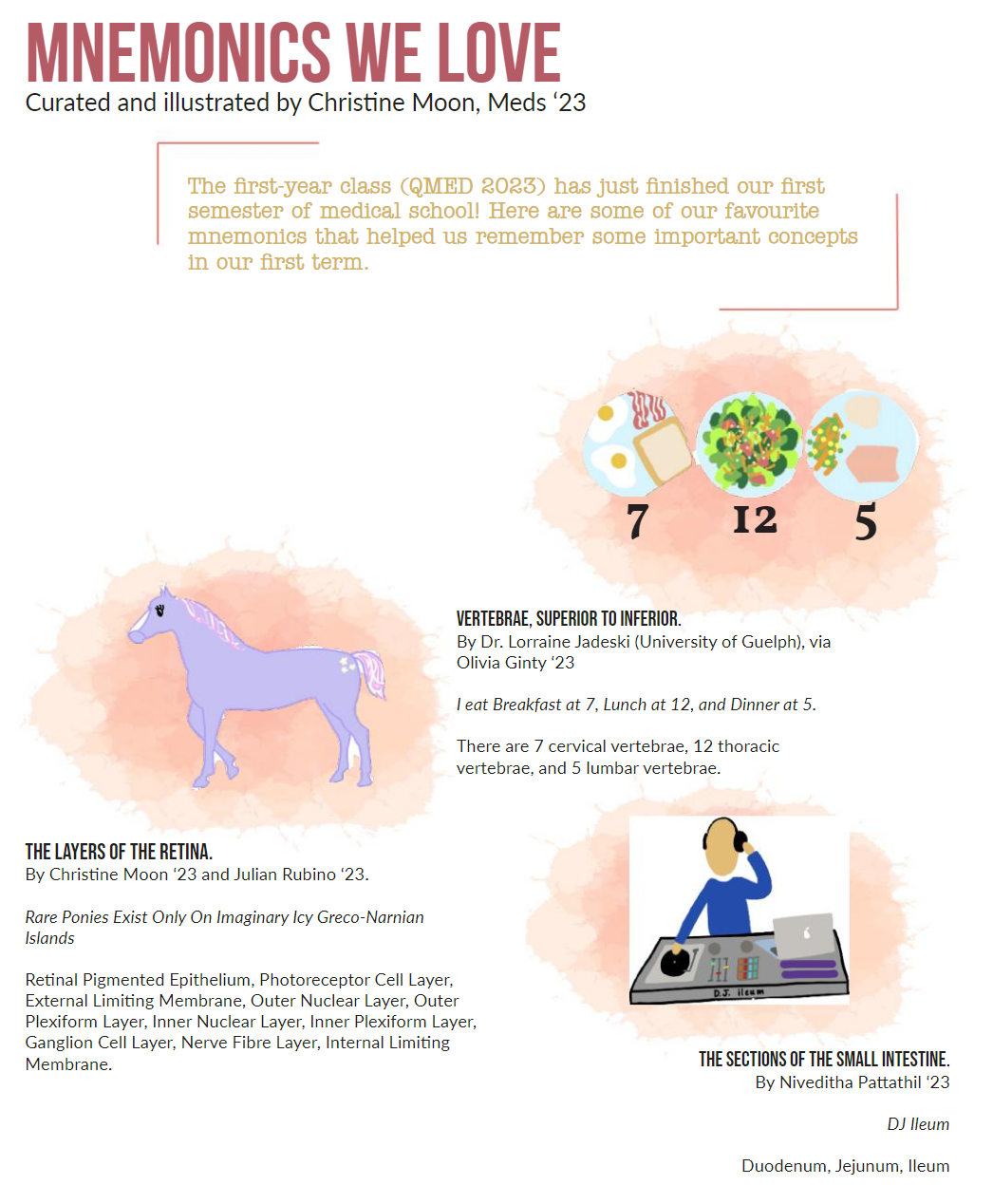
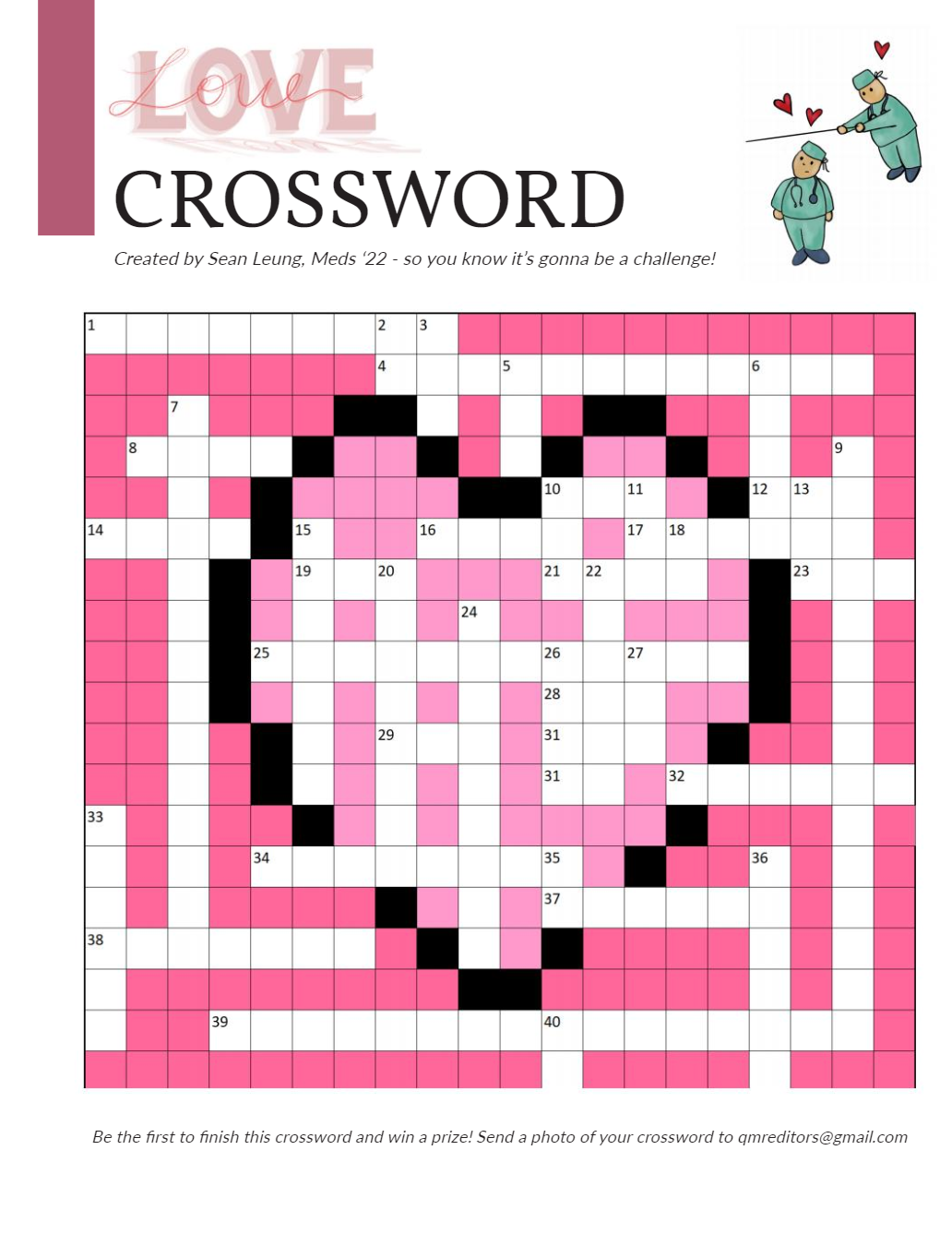
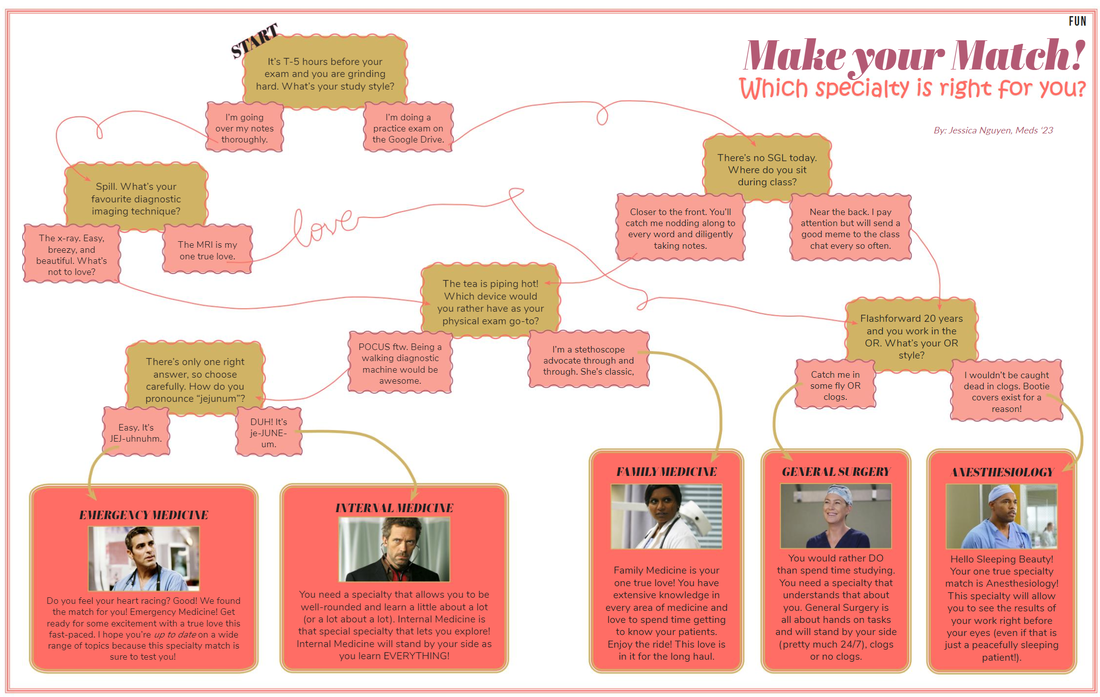
Dear lovely readers, Welcome to our Love issue. We are so thrilled that you have decided to pick up a copy of the QMR and give it a read. We are very proud of the content that our entire team (writers, editors, layout, and artists) have brought forward to this issue. For this issue, we challenged the Queen’s Medicine community to interpret the theme of Love (in medicine) in various ways. Given the dynamic spread of talent in the QMed community, it should come as no surprise that the results were wide-ranging. In The Importance of Love and Human Connection in Medicine, Karthik Manickavachagam speaks to the human element of medicine and explains how we can facilitate more meaningful interactions in the hospital setting. Meanwhile, Andriy Katyukha presents the argument that while Electronic Patient Records might make things more efficient in the hospital, they can also serve to create barriers between patients and care providers in Patient Centered Care? In Humanity, Love, and Medicine, Iku Nowsu encourages us to challenge constructs about how we express and speak about “love” in medicine. We also are offered insight into the experience that two students shared with their First Patient in a deeply touching article about “Stanley”. In addition to reflections on love, we also offer up conversations about the heart as its own entity. Emma Spence takes a literal look at what it might mean to suffer from a broken heart in Takotsubo Cardiomyopathy/Broken Heart Syndrome while A Case for Wearing Your Heart on Your Sleeve explores what it means to bring your heart to the forefront in a metaphorical sense. Alex Morra also renders a beautiful poem, Patent Foramen Ovale, which speaks to what it means to have a heart that is open. This issue is ripe with deep and meditative insights on love in medicine, and we also offer up some light and fun fare. We have another thematic crossword for you, with a prize for the person who completes it first (contact [email protected])! Additionally, Christine Moon has curated a number of helpful Mnemonics We Love to aid with memorization during the dreaded second semester slump. If you have been feeling introspective, you can check out the Specialty Love Map, created by Jessica Nguyen, which might guide you toward your career soul mate, or you could also check our your Love Horoscope, if you are wondering about compatibility with a real life mate. Once again, we are so excited to share another round of Dear QMR, wherein anonymous upper-year students answer questions submitted by members of the QMed community. We are so thankful for the contributions from all of you. We hope that this column is both fun, powerful, and emotional all-at-once! A special acknowledgment goes out to our hard-working managing editors, Grace Yin and Christine Moon, who have been pulling strings behind the scenes for the past couple of months, our content editors, Zoe Hu, Jessica Nguyen, and Sarenna Lalani for making sure we have all crossed our t’s and dotted our i’s (and also for making us all sound better), and to our phenomenal artistry and layout team: Amanda Mills, Doan-Nghi Dam-Le, Jessica Nguyen and Andrew Lee who have done a stellar job making the QMR look lovely. A special shout-out goes to Simran Sandhu for her amazing collage piece that is featured as the cover of this issue! Whatever it is you seek out - we hope there is something for you in this issue. We thank you for taking the time to support our creative endeavor, and to all of those who have contributed in their many ways. It takes a village, and we happen to reside in the best one out there. Nicole Krysa & Kimberley Yuen 
0 Comments
By Harry Chandrakumaran, Meds '20  February Love Horoscopes
Amanda Mills, Meds '23 Pisces: This is your month Pisces! We know you love to show your emotions, especially around Valentine’s Day. With Mercury in pisces this month you will meet new people very easily – maybe think about giving a new friendship, mentorship, or relationship a chance. Aries: Although this month may seem long and arduous, with resolutions to keep and work to keep up on, you’ll have the ability to handle these pressures with relative ease. Make sure to continue to pay attention to those around you, they may need your love and support this month! Taurus: This February you’ll have increased willpower and persistence. Mercury in Pisces will allow you to improve your communication skills with those around you. Use your determination and these communication skills to have the conversations you want to! Gemini: Winter is almost over, Gemini! Use your friendly and sympathetic attitude this month to stay open-minded to the opinions of those around you. There’s no better time than this month to learn something from someone you love! Cancer: This month is all about romance for you, Cancer! For you, the strong influence of Venus in Pisces will allow for ease in getting along with others. Use this to your advantage and enjoy spending time with your loved ones! Leo: This month you will embrace your passionate side to stand up for what you believe in. Don’t be afraid! Just be honest with yourself and step into your thoughts, feelings, and opinions. Virgo: You will be overflowing with ideas this month. Follow your heart and explore what these ideas have to offer! Enjoy this burst of creativity and write down anything that comes to mind. You may need these ideas later ;) Libra: Libra, February is all about respect for you. Make sure you respect yourself and everyone around you as you make your way through this frosty month. It’s time to show some love to yourself and take care of YOUR needs! Scorpio: You may find yourself distracted this month, Scorpio. Lean in! It’s okay to focus on dreams of the future this month. Stay true to your heart and think about what makes it beat faster. You’ll have lots of energy this month, so keep daydreaming! Sagittarius: Welcome to February, Sagittarius! This month is all about warmth and positivity for you. Spread the love! You will find boundless energy, confidence, and interesting ideas you’ll want to share with those around you. Capricorn: With Mars in Sagittarius, you may feel inclined to throw yourself into your work this month, Capricorn. That’s okay! Take the time to do what you love, especially when you’re feeling passionate about it. It’s okay if you take some time alone to focus – just make sure you keep checking in with your support system. Aquarius: Listen to your body this month, Aquarius! You may feel like you have endless energy this month, but make sure you take time to rest and catch up with those you love. With Mercury in Pisces, you will have the opportunity to deepen relationships this month – take it! Iku Nwosu, Meds '22“I love our patients” is a routine statement from healthcare professionals and students. It is a statement so common it rarely packs a punch. Love is funny in medicine. Funny because we will hopefully love our patients, and love what we do; love can define that feeling of fulfillment we yearn for. Yet, love can also seem so indisputably inappropriate.
Spin love differently - by telling a patient you love them. The thought can leave you tongue-tied. Suddenly it feels so wrongly direct, across a line that we have created for ourselves. Now, I am not denying the importance of this line and the problems that would arise without it. And no, I do not foresee or encourage a future where we express our love to patients explicitly in the wards. I am simply acknowledging love, humanity, and medicine intertwined. Given love plays such a transformative role in medicine, perhaps we should challenge this boundary we have created for ourselves in pursuit of better patient care. “Pearls” in medicine are almost never about medicine in the literal sense - or at least the really good ones. Some great ones I’ve received are simple lessons: be generous with your patients; remember the reason you chose medicine; do not make assumptions of patients and their stories. It is uncanny how many of them relate back to virtues; kindness, compassion, and remarkably - love. People show love in medicine as part of an unconscious routine. It speaks to the humanity that persists, and lacking in it is just not an option. Medicine catches people on their best and worst days, or somewhere in between. To be impactful on any of these days, anywhere on this spectrum, people need to feel like you feel something. People respond to love. Despite this natural unease that can surround the concept of love, people accept it. Medicine is filled with anecdotes; the experiences we have in healthcare become the stories we talk about. Growing up, I watched my parents love seeing our family physician. Their need to get a prescription refilled also came with a true desire to catch up with someone they considered a friend. These impressions made by a healthcare professional are seen across patients, from the most debilitating illness experiences to the ongoing relationships in primary care. We very unsubtly do a disservice to those who cannot share the same sentiments. Not everyone loves going to the doctor – we see that for many the system can feel unwelcoming and rooted in hostility. Our feelings about a place and its people, and our perception of their feelings towards us will direct how often we go to it. Acknowledging this tongue-tied feeling around a concept like love in medicine, is acknowledging a part of our humanity. It is unlikely much will ever change about how we talk about love in medicine; in many ways these boundaries keep people safe. Perhaps, in the future we will play with these boundaries as humans, as we slowly recognize what complex beings we are in a world changing so quickly around us. Love and medicine cannot be separated because love and humanity cannot be separated. ANDRIY KATYUKHA, MEDS '22Cursory assessment would lead one to prematurely, and dare I say, erroneously, conclude that the Electronic Patient Record (EPR) plays a positive role in improving patient care. Dissenters would be chastised by the majority of people who see the EPR as a centralized reservoir that contains vital details pertaining to a patient’s journey through the healthcare system. It is argued that such details are important in understanding medical presentations and collating the summation of interpretations by practitioners far and wide. I would be remiss to not acknowledge that details and facts are the basis of medical reasoning, and following that logic, a complete electronic account would lead to increased accuracy in the treatment of patients.
I argue, however, that a complete account is not synonymous with an accurate account. In the most elementary sense, I equate the EPR to a telephone system, via which information is transmitted. Let’s now add some complexity to this system. Each entry in the EPR represents a transmission point, where information is hopefully sent across in its totality to create a sufficient account of “the patient experience”. It is then propagated down the system until it is accessed by an overworked, idealistic resident working an overnight shift in a busy academic centre. The record in the EPR is sacrosanct, and oftentimes not questioned because questioning leads to inefficiency, thus undermining the very goal of this “invaluable system”. The amount of times that incomplete and inaccurate information is scribed into the EPR is too many to count. Our superior communication system quickly deteriorates into nothing more than a broken telephone. It is quite obvious that decisions made on seemingly correct, yet wildly inaccurate information, lead to dismal patient outcomes. This reliance on the EPR limits the need for a proper patient led account of an incident, as the information needed for diagnosis has already been collected and rehashed by multiple providers. Why ask the same questions again, if you already have a complete account of the issue presented to you? This function fundamentally undermines what healthcare providers are taught to do—talk to their patients. Conversations become abrupt, and the EPR fills in the details. The model of patient-centered care is slowly eroded and what is left in its place is EPR centered care. This care is detached, hollow, and predicated on a “patient-less” experience. By Emma Spence, MEDS '21While we may not be able to physically “laugh our head off” or “cry our eyes out,” can someone really “die of a broken heart?” Perhaps the answer is yes.
Broken Heart Syndrome, or more formally Takotsubo Cardiomyopathy, is described as transient dysfunction of the left ventricle (LV) in the absence of significant coronary artery disease. On echo, the resulting regional myocardial dysfunction leads to a systolic ballooning appearance of the LV apex. The etymology of the term “Takotsubo” stems from a Japanese pot used as an octopus trap, the shape of which is similar to the echocardiographic or radiographic appearance of the LV abnormality in the most typical form of the condition. But how did this disease earn its melancholic alias? Well, while there remains uncertainty as to the exact etiology and pathogenesis of this phenomenon, emotionally stressful events such as a traumatic break-up or unexpected sudden loss of a loved one are commonly associated triggers. The presenting symptom is most often retrosternal chest pain, but patients can present with dyspnea or syncope. Symptoms of heart failure may also ensue. Auscultation may reveal new murmurs pointing toward acute mitral regurgitation or dynamic LV outflow tract obstruction. Cardiac biomarkers and ECG findings are often similar to STEMI with elevated troponins, ST elevation, T wave inversion and abnormal Q waves. However, angiography will not show significant obstructive coronary artery disease or acute plaque rupture (though it is possible to have co-morbid CAD that may or may not be contributing to the presentation). Ventriculography or echo will demonstrate the LV wall abnormality (the octopus trap), and the latter is performed in serial fashion to follow along for resolution. Given that stress cardiomyopathy and its complications can be life threatening, perhaps we really can die of a broken heart. However, the events themselves do tend to be transient, meaning that perhaps our mothers are, as always, right – only time can mend a broken heart. Sources: UpToDate. Reeder, G.S., Prasad, A. Clinical manifestations and diagnosis of stress (Takotsubo) Cardiomyopathy. In: UpToDate, Post, TW (ed), UpToDate, Watham, MA, 2019 DynaMed. Takotsubo Syndrome. In: DynaMed, Ipswich, MA, updated Nov 30, 2018 By Karthik Manickavachagam, MEDS '22When Mother Theresa visited the United States, she gave a speech in which she emphasized the importance of love and human connection. She reflected that in developing countries there was indeed poverty – a poverty of money – but that in developed countries there was a greater poverty – a poverty of love. She explained that when she visited nursing homes in developed nations, she found the residents wanting for love and human connection. As doctors-in-training and future physicians, we have the power to address this issue within the realm of healthcare. In addition to addressing the physiologic ailments of patients, it is important that we foster a human connection based on love and compassion, because after all, patients are not machines that we fix but rather, humans that we heal.
One powerful tool which we can use while striving to heal patients is the human smile. I learned this poignant lesson from a dying cancer patient as a second-year nursing student. I was nervous and unsure of how to interact with a dying patient. However, the patient put me at ease with her smile and small talk. Even now, years after this encounter, I remember how a simple smile made the interaction more comfortable and meaningful. Another way to enhance the therapeutic relationship is to listen with undivided attention and to be ‘fully present’ during interactions with patients. This can be challenging with the multitude of demands placed on healthcare providers, not to mention the numerous smart phones and pagers constantly going off. However, a physician who is not ‘present’, hinders the therapeutic relationship and leaves patients feeling unimportant and uncared for. One thing I have noticed good physicians do is excuse themselves to attend to an important phone call and then return to the patient with their undivided attention. This not only improves the patient experience but, as a bonus, reduces medical errors. Often the nature of our conversations with patients and their family members involves difficult topics such as choosing palliative care and forgoing futile aggressive treatments. Fittingly, during these conversations, many emotions arise. While it is important that we do not become over attached to patients, we still have a duty to support them and be part of a genuine conversation. Holding their hand and sitting in silence (despite the urge to fill it up) are powerful techniques to support patients and build connection. To conclude, human connection is integral to establishing a therapeutic relationship and providing good medical care to patients. Use of the above techniques and keeping an open mind to learn from others can help us achieve this important goal. |
In this Issue:
All
|
 RSS Feed
RSS Feed
